Key takeaways:
- Lung function was defined by ratio of time to peak tidal expiratory flow to expiratory time.
- Skin barrier impairment was defined as transepidermal water loss of 9.5 g/m2/hour and higher.
Young infants with lower lung function and impaired skin barrier function experienced greater risks for developing asthma by age 3 years, according to a study published in Allergy.
These associations differed by sex, among other factors, Martin Färdig, MSc, PhD student, department of women’s and children’s health, Karolinska Institutet, and colleagues wrote.
Data were derived from Färdig M, et al. Allergy. 2024;doi:10.1111/all.16024.
The Preventing Atopic Dermatitis and ALLergies in children mother-birth cohort included 1,337 children (52.5% boys) with mean ages of 3.1 ± 0.3 months at their 3-month clinical follow-up and 3.2 ± 0.3 years at their 3-year clinical follow-up.
Among 563 infants with lung function data at age 3 months, mean ratio of time to reach peak tidal expiratory flow (tPTEF) to exploratory time (tE) was 0.39 ± 0.08 seconds with a tPTEF of 0.2 ± 0.05 seconds.
The researchers characterized 30 (5.3%) infants with lower lung function based on their tPTEF/tE of less than 0.25 seconds and 139 (24.7%) infants with lower lung function based on their tPTEF of less than 0.17 seconds.
Also at age 3 months, 1,173 infants whose skin barrier function had a mean transepidermal water loss (TEWL) of 8.4 ± 6.1 g/m2/h. The researchers characterized 294 (25.1%) of these infants with TWELs higher than 9.5 g/m2/hour with impaired skin barrier function.
Further, 168 of 1,318 (12.7%) infants had eczema at age 3 months, and 96 of 1,045 (9.2%) had an FLG mutation.
Overall, 180 children in the full cohort (13.5%) had asthma at age 3 years, defined as three or more episodes of bronchial obstruction between ages 2 and 3 years in addition to a history of doctor diagnosis and asthma medication use.
At age 3 years, 137 of 167 children with asthma (82%) also had a parent with a history of atopy, compared with 685 of the 1,084 children who did not have asthma (63.2%; P < .001).
Although 524 children in the full cohort (39.2%) had lower tPTEF/tE or shorter TPTEF with high TEWL, eczema or FLG mutations at age 3 months, none of them had all four conditions. However, the researchers wrote, there were associations between high TEWL, eczema and FLG mutations and between tPTEF and high TEWL.
By sex, 122 of 702 boys (17.4%) and 58 of 635 girls (9.1%) had asthma at age 3 years (P < .05). Mean tPTEF/tE results included 0.38 ± 0.08 for boys and 0.4 ± 0.08 for girls (P < .05). Similarly, mean tPTEF results included 0.2 ± 0.05 for boys and 0.21 ± 0.05 for girls (P < .05).
Boys and girls also had similar mean TEWL, rates of eczema and FLG mutations.
The researchers characterized distributions of tPTEF/tE, tPTEF, TEWL and eczema at age 3 months and FLG mutations and asthma at age 3 years among the included children and the remaining cohort as similar, but allergic sensitization and atopic dermatitis at age 3 years were not.
Specifically, 68 of 180 children with asthma (37.8%) were diagnosed with allergic sensitization and 51 of 179 children with asthma (28.5%) were diagnosed with AD by age 3 years.
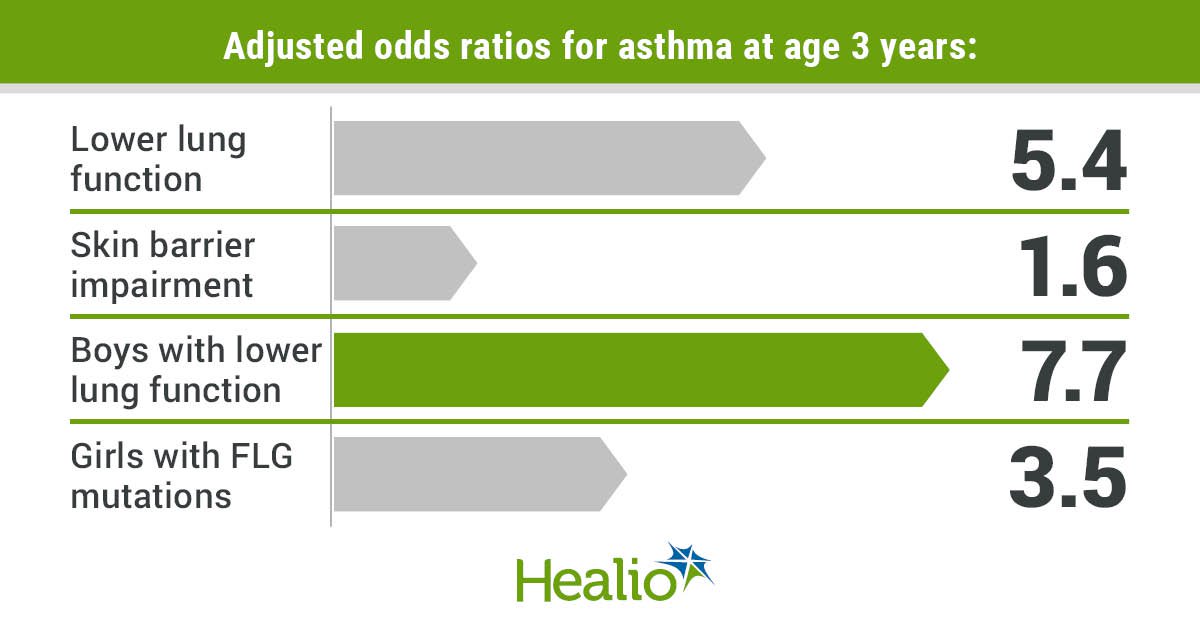
There also were associations between asthma and lower tPTEF/tE (adjusted OR = 5.4; 95% CI, 2.1-13.7), shorter tPTEF (aOR = 2.7; 95% CI, 1.5-4.9), and high TEWL (aOR = 1.6; 95% CI, 1.1-2.5) but not between asthma and eczema or FLG mutations at age 3 years.
Boys experienced significant associations between asthma and lower tPTEF/tE (aOR = 7.7; 95% CI, 2.5-23.6) and shorter tPTEF (aOR = 3.2; 95% CI, 1.5-6.7) but not between asthma and high TEWL, eczema or FLG mutations at age 3 years.
Girls experienced associations between asthma and FLG mutations at age 3 years (aOR = 3.5; 95% CI, 1.5-8.2) but not between asthma and any of the other conditions that were studied.
Although lower lung function had an independent association with asthma at age 3 years, the researchers said, high TEWL only was associated with asthma among children diagnosed with AD (aOR = 3.4; 95% CI, 1.8-6.4) or allergic sensitization (aOR = 6.8; 95% CI, 3.1-14.9) at age 3 years.
Asthma additionally was associated with eczema in children with AD (aOR = 3.2; 95% CI, 1.6-6.1) and allergic sensitization (aOR = 3.3; 95% CI, 1.6-6.8) and with FLG mutations in children with AD (aOR = 2.5; 95% CI, 1.2-5.2) and with allergic sensitization (aOR = 2.7; 1.2-6.1) at age 3 years.
Shorter tPTEF predicted asthma with 44.6% sensitivity and 78.3% specificity with a receiver operating characteristics-area under the curve of 0.62 (95% CI, 0.54-0.69) at age 3 years, but the skin conditions that were studied did not, the researchers said.
Based on these findings, the researchers concluded that lower lung function and impaired skin barrier function at age 3 months increased risks for asthma at age 3 years, but FLG mutations and eczema at age 3 months did not.
These results also suggest that epithelial barrier function may play a role in asthma development by age 3 years and that the progression from reduced skin barrier function to allergic inflammatory conditions are important in asthma development.
Perspective

I do not think these findings are too surprising or significant. I think the idea of measuring lung function as early as 3 months and association of asthma later in life (3 years) may not be too surprising. Another group showed very similar results in a previous publication. In addition, as the authors point out, similar findings for other parts of this study have largely been reported before.
I don’t personally do research in this area, so my experience is limited to clinical experience. In the clinic, we use tools to help us predict asthma in infant wheezers. For example, things such as the Asthma Predictive Index were developed to help us try to predict which infant wheezers will have asthma later in childhood. That is similar to this study. However, this study looked at physiologic markers (lung function and TEWL) very early on to help predict asthma at 3 years of age (in healthy infants).
It would be very hard to use these results to do anything with patient care. No one is clinically using the assessment of lung function at 3 months of age. In addition, I don’t know anyone looking at TEWL in a regular clinical setting. Thus, as the authors point out in their discussion: “Consequently, our results are likely to be relevant to further understand the role of lung and skin barrier function in early infancy and young children developing asthma, rather than being useful in a clinical setting.”
Thus, this is really just one small piece in the bigger exploration of this birth cohort study, which is to better understand what factors in infancy are associated with asthma and allergies and how can we possibly intervene early to affect the outcome. However, nothing in this report will change that.
We need to await the actual outcome results of the larger birth cohort study. There also are similar studies going on worldwide, such as the Seal, or Stopping Eczema and Allergy study, for example, looking at how we can change outcomes in these infants who have eczema early on.
Reference:
Håland G, et al. N Engl J Med. 2006;doi:10.1056/NEJMoa052885.
Seal, Stopping Eczema and Allergy Study. https://clinicaltrials.gov/study/NCT03742414. Published Oct. 26, 2023. Accessed May 6, 2024.
Jay A. Lieberman, MD
Associate Professor, University of Tennessee Health Science CenterMember, Healio Allergy/Asthma Peer Perspective Board
Disclosures: Lieberman reports having investigator roles with Aimmune Therapeutics, DBV, Novartis and Regeneron; having data safety monitoring board roles with AbbVie and Siolta; having advisory board roles with ALK, Aquestive Therapeutics, DBV and Novartis; and serving as an associate editor for Annals of Allergy, Asthma & Immunology and as an executive board member for the American Board of Allergy and Immunology.
Sources/Disclosures
Collapse
Färdig M, et al. Allergy. 2024;doi:10.1111/all.16024.
Disclosures:
Färdig reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures.