In a recent study published in the journal The Lancet Public Health, researchers examined the differences in the leading causes of disease burden between males and females.
Evidence shows that females outlive males despite experiencing a higher degree of non-fatal conditions; this phenomenon is called the male-female health-survival paradox. Further, it has been recognized that gender and sex interact with various factors (e.g., ethnicity/race, age, sexual orientation, socioeconomic status) in shaping human health.
Sex refers to the biological factors linked with physiological and physical traits (sex chromosomes, reproductive anatomy, and hormones). Meanwhile, gender relates to socially constructed roles, behaviors, and identities of males, females, and gender-diverse individuals. These dynamic, intertwined social and biological processes may lead to males, females, and sex- and gender-diverse people experiencing health and disease differently.
Differences across the lifespan between females and males in the top 20 causes of disease burden globally: a systematic analysis of the Global Burden of Disease Study 2021. Image Credit: Hyejin Kang / Shutterstock
About the study
In the present study, researchers investigated the differences in the leading causes of disease burden between males and females. They used data from the Global Burden of Diseases, Injuries, and Risk Factors (GBD) 2021 study, which reported morbidity and mortality estimates between 1990 and 2021 across 204 countries and territories.
These estimates were used to quantify the differences in the leading causes of disability-adjusted life years (DALYs) between males and females worldwide. DALYs were estimated as the sum of years lived with disability and years of life lost due to premature mortality. DALY estimates were available for males and females for 20 age bands from early childhood to ≥ 95 years for 204 countries and territories.
The GBD study organized diseases and injuries along a four-level hierarchy of causes. The present study focused on level 3 as the primary outcome. Level 3 causes were globally ranked according to the age-standardized rates of DALYs per 100,000 people aged ≥ 10 in 2021. The researchers focused on the top 20 leading causes from this ranking.
Descriptive analyses were performed to determine the differences in cause-specific DALY rates. Findings were reported for five age groups. DALY rates were available for middle-aged (50–69) and older (≥ 70) adults, while for the 10–24 and 25–49 age groups, standard five-year DALY rates were aggregated using GBD population estimates.
For the aged-standardized group (≥ 10 years), GBD global population age standard weights were used to estimate DALY rates. The team explored relative and absolute differences in DALY rates between the two sexes by cause across seven ‘super-regions’ and worldwide. The relative contribution of morbidity and premature mortality to the disease burden was also examined.
Findings
The age-standardized DALY rates were higher for males for 13 causes and females for seven causes in 2021. The seven causes among females included low back pain, headache, depressive disorders, anxiety, other musculoskeletal disorders, human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), and dementia. Most of these conditions were ranked within the ten leading causes of female disease burden in 2021.
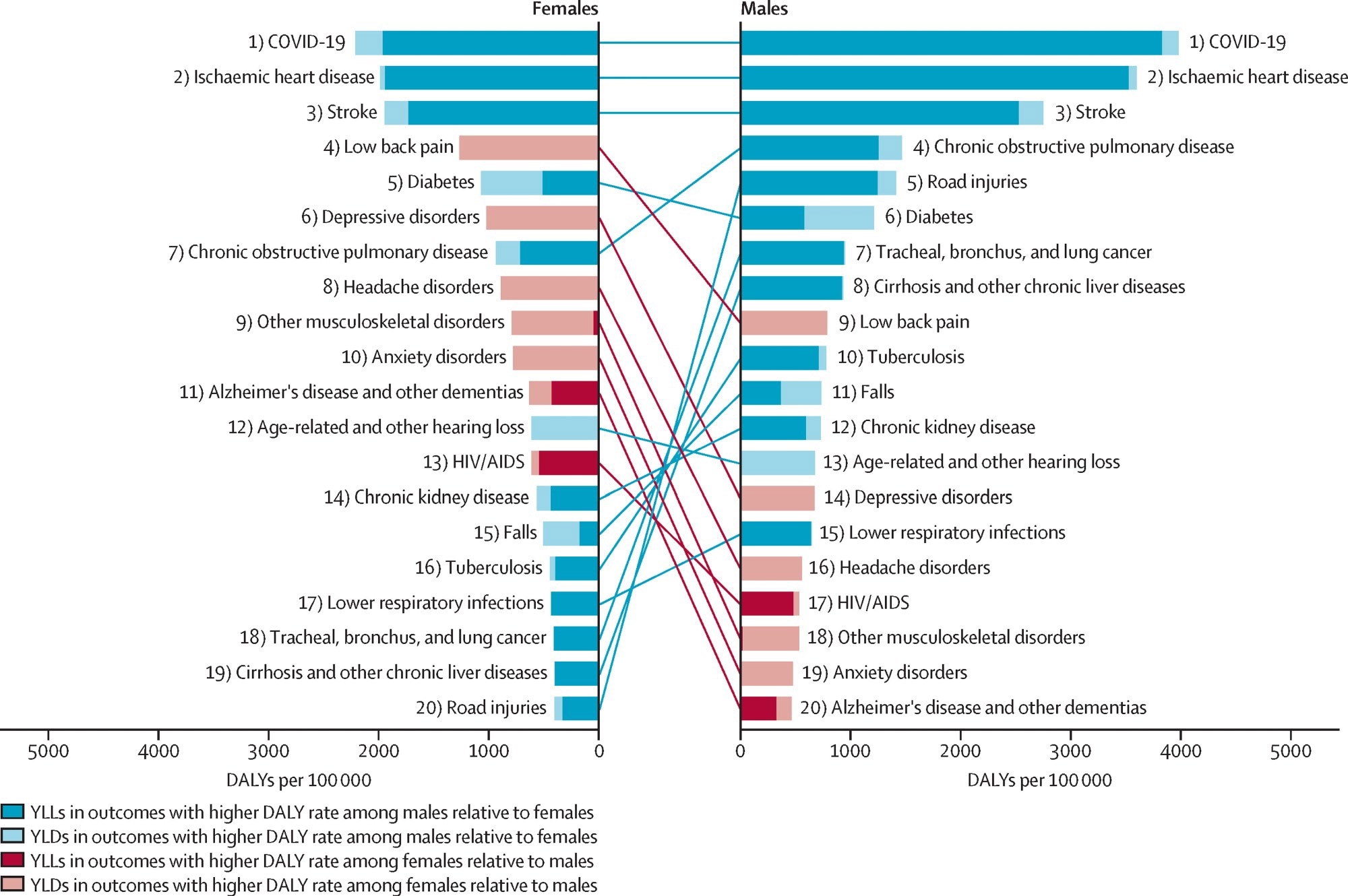
Global rankings of the top 20 causes of DALYs globally for females and males, age-standardised (10 years and older), 2021. The list of causes of disease burden represents the top 20 causes of age-standardised DALYs observed across females and males for the age group of 10 years and older globally in 2021. This same list of health conditions was ranked according to the DALY rates (per 100 000 population) for both females and males globally in 2021 for the same age group. The colours of the bars and lines denote whether DALY rates are higher for females (red) or males (blue) as established by whether the 95% uncertainty interval of the absolute difference in DALY rates includes zero. The degree of transparency reflects the composition of DALYs for each cause, split between mortality (YLL) and morbidity (YLD). DALY=disability-adjusted life-year. YLL=years of life lost. YLD=years lived with disability.
Morbidity accounted for much of the burden for causes with increased DALY rates in females, while premature mortality contributed substantially to that among males. Low back pain had the largest absolute difference, with over 478 more DALYs per 100,000 females in 2021 than males. Anxiety had the highest relative difference, with 64.8% increased rates among females relative to males.
Among males, coronavirus disease 2019 (COVID-19) had the most significant absolute difference in 2021, with 1767.8 more DALYs per 100,000 males than females. Further, road injuries had the largest relative difference. For conditions wherein females had higher DALY rates than males, the differences between the two sexes emerged early in life. Conversely, for conditions wherein males had a higher burden than females, the differences between the sexes were minor at early ages.
With a few exceptions, the absolute differences in age-standardized DALY rates between males and females gradually changed between 1990 and 2021. However, the absolute differences for tuberculosis, Alzheimer’s disease and other dementias, cirrhosis and other liver diseases, ischemic heart disease, and chronic kidney disease remained the same. Notably, HIV/AIDS exhibited considerable temporal variations.
Conclusions
Taken together, the findings indicated that males had a higher overall disease burden in 2021, while females had a higher burden of seven causes. Notably, the differences emerged early in life, a phase characterized by pubertal changes and gender socialization, highlighting the need for early response. They continued to widen with age for several conditions. The study highlights the significance of adopting a life-course approach in strategic planning. The approach should comprise early, tailored interventions to prevent the onset and aggravation of specific health conditions throughout life.