Key takeaways:
- Individuals with breast cancer most often declined chemotherapy compared with other modalities.
- Black patients more often declined surgery and radiotherapy compared with other groups in the study.
Racial and ethnic minorities with breast cancer had a higher likelihood of declining various treatment options than white patients in the past 2 decades, results from a retrospective study published in JAMA Network Open showed.
Individuals who received chemotherapy, hormone therapy, radiotherapy and/or surgery had higher 5-year and 10-year OS rates than those who did not, according to study investigators. Moreover, they observed a trend showing significantly more patients declining treatment with hormone therapy, radiotherapy or surgery.

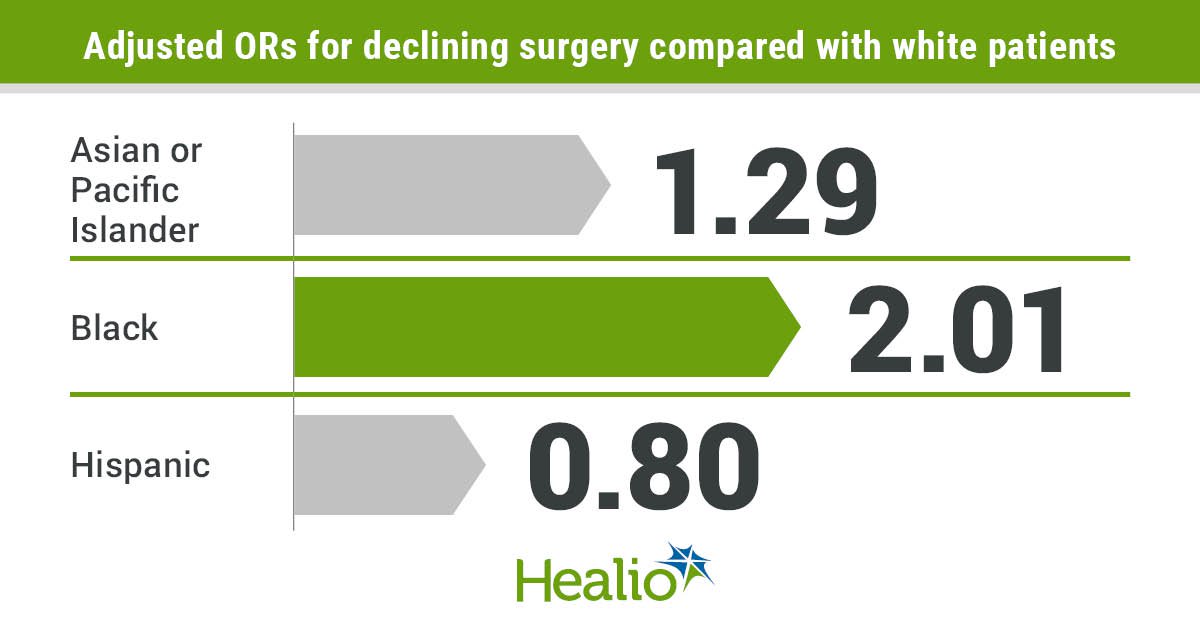
Data derived from Freeman JQ, et al. JAMA Netw Open. 2024;doi:10.1001/jamanetworkopen.2024.9449.
“These findings highlight racial and ethnic disparities in treatment declination and overall survival of patients with breast cancer, suggesting that equity-focused interventions are needed to address the disparities to improve patients’ survival,” researchers wrote.
Background and methodology
Healio previously reported an American Cancer Society estimate that breast cancer, among all cancer types, would account for the highest number of newly diagnosed cancer cases in the U.S. this year, with 313,510. The same report noted breast cancer would cause 42,780 deaths.
“Breast cancer diagnosis and treatment can take a heavy toll on patients’ physical, mental, psychosocial and financial health,” Jincong Q. Freeman, MPH, MS, graduate student at the University of Chicago, and colleagues wrote.
“Some patients with cancer choose to decline treatment despite clinician recommendations and treatment benefits,” they added. “Declining curative treatment can have a detrimental effect on these patients’ short-term and long-term health outcomes and quality of life.”
Researchers noted previous studies had concluded individuals with any cancer who declined treatment had higher risk for mortality than those who accepted it. Additionally, the decision to decline treatment had links to various sociodemographic and clinical factors.
Freeman and colleagues wanted to take their investigation further and investigate national trends in treatment declination and factors associated with those choices, as well as evaluate any impact on OS among different racial and ethnic groups.
They conducted a cross-sectional analysis using information from the National Cancer Database from 2004 to 2020.
The study cohort included 2,837,446 individuals (mean age, 61.6 years; 99.1% women), with a demographic breakdown of 78% white; 11.2% Black; 5.6% Hispanic; 3.5% Asian or Pacific Islander; and 1.7% American Indian, Alaska Native, or other.
Researchers also divided the study cohort into four smaller subsets based on treatment type — chemotherapy, hormone therapy, radiotherapy and surgery.
Results and next steps
Most patients (89.9%) received all their recommended treatments.
Patients declined chemotherapy more than any other treatment (9.6% of those offered), followed by radiotherapy (6.1%), hormone therapy (5%) and surgery (0.6%).
Radiotherapy, hormone therapy and surgery all had increasing trends of declination between 2004 and 2020, while chemotherapy saw a decrease in refusal.
In the chemotherapy cohort, more white patients declined treatment than other racial and ethnic groups, but after a covariate adjustment, American Indian, Alaska Native, or other; Asian or Pacific Islander; and Black patients all had a higher likelihood of declining therapy than white individuals.
Black patients who declined chemotherapy had a higher mortality risk than white individuals (adjusted HR = 1.07; 95% CI, 1.02-1.13).
In the radiotherapy cohort, white and Black patients had the highest rates of declination, but after multivariable analysis, Black patients had a higher likelihood of refusing therapy than white patients.
In the surgery cohort, Black individuals had the highest declination rates, and they — along with American Indian, Alaska Native, or other; and Asian or Pacific Islander patients — had greater odds of declining treatment than white individuals.
In the hormone therapy cohort, white individuals had a higher percentage of declination and increased likelihood compared with American Indian, Alaska Native, or other; Asian or Pacific Islander; and Black patients.
Older age, uninsured patients and those with Medicaid (compared with privately insured individuals) had higher likelihood of declining therapy for all four treatment options.
Individuals insured through Medicare had a higher likelihood of refusal for radiotherapy, and lower income households had increased odds for declining therapy in the chemotherapy, radiotherapy and surgery groups.
Hispanic patients had a lower likelihood of declining chemotherapy, radiotherapy and surgery than white individuals.
Tumor stage and grade factored into declination rates as well for all four treatment options.
Study limitations included potential underreporting of data and unstudied factors such as marital status and religious beliefs.
Researchers stressed the need for interventions that focus on patient education about the benefits of treatment and enhancing the patient-physician relationship to improve patient outcomes and reduce racial and ethnic disparities.
“To encourage patients to accept recommended cancer care, policies to reduce financial and logistical barriers, such as paid sick leave and universal health insurance with low cost-sharing for financially toxic diagnoses, could be implemented,” Gregory S. Calip, PharmD, MPH, PhD, adjunct associate professor at University of Southern California, and colleagues added in an accompanying editorial.
“These policies would enable patients to choose treatment rather than being forced to forgo care due to financial or logistical barriers to comprehensive cancer care,” they wrote. “Culturally sensitive patient education on treatment benefits, improved patient-clinician communication, and shared decision-making should also be prioritized to ensure that all patients, regardless of race or ethnicity, feel empowered to make informed decisions about their care.”
References:
Sources/Disclosures
Collapse
Disclosures:
Authors of the study report no relevant financial disclosures. Calip reports grants from Pfizer and personal fees and stock ownership from AbbVie. Please see the editorial for all other authors’ relevant financial disclosures.