Key takeaways:
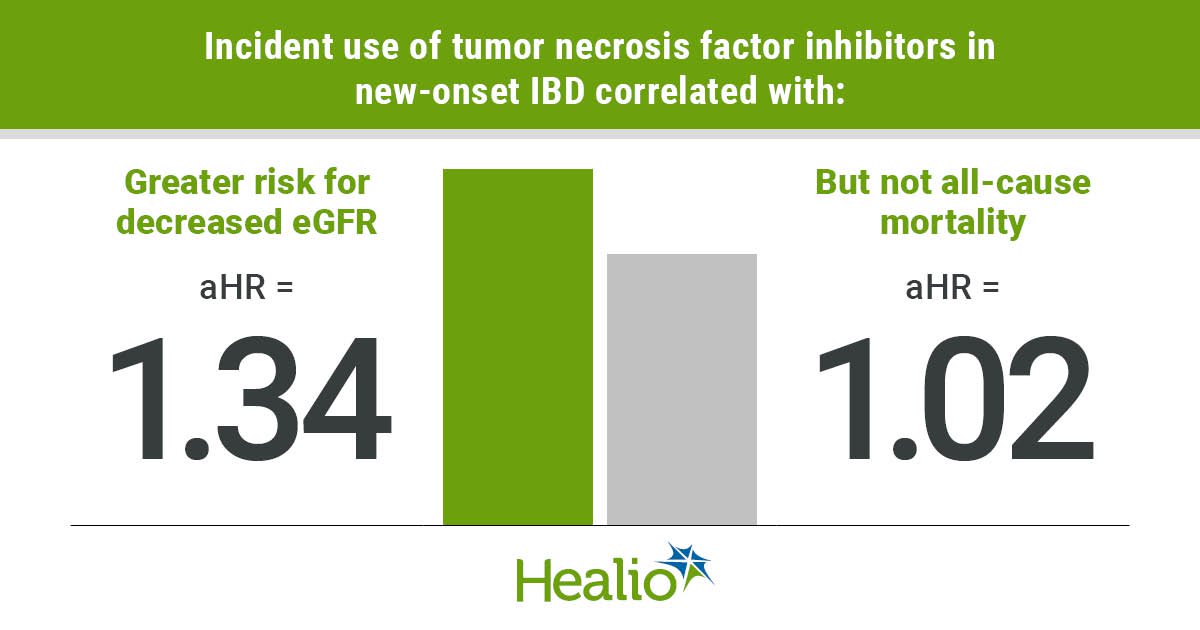
- Anti-TNF use was significantly associated with higher risk for progressive kidney function decline among patients with new-onset IBD.
- It was not associated with risk for all-cause mortality.
Tumor necrosis factor inhibitor use was independently associated with a greater risk for progressive kidney function decline but not risk for all-cause mortality among patients with new-onset inflammatory bowel disease, according to data.
“To date, a number of studies have reported favorable effects of anti-TNF therapy on the extraintestinal manifestations of IBD,” Keiichi Sumida, MD, MPH, PhD, of the division of nephrology at the University of Tennessee Health Science Center, and colleagues wrote in JAMA Network Open. “Despite this, studies investigating the effect of anti-TNF therapy on survival for patients with IBD are limited, and to our knowledge, no prior studies have assessed its effect on the risk of CKD progression, a well-known extraintestinal manifestation of IBD and an established risk factor for mortality, in these patients.”

Data derived from: Sumida K, et al. JAMA Netw Open. 2024;doi:10.1001/jamanetworkopen.2024.6822.
Using data from the Therapeutic Interventions to Assess Outcomes and Disparities in Chronic Kidney Disease (CKD) study — a nationwide cohort of more than 3.5 million U.S. veterans — researchers assessed whether anti-TNF therapy was associated with kidney disease progression and mortality among 10,689 patients (mean age, 67.4 years; 93.5% men) with new-onset IBD between October 2004 and September 2019. They noted 31.4% of patients had diabetes, 14.2% were newly initiated on anti-TNF therapy and the mean estimated glomerular filtration rate (eGFR) was 77.2 mL/min/1.73 m2 at baseline.
Primary outcomes were at least 30% decline in eGFR and all-cause mortality.
According to study results, 3,337 patients — 607 anti-TNF users and 2,760 nonusers — experienced at least 30% decline in eGFR during a median follow-up of 4.1 years, and 2,502 patients died over a median follow-up of 5 years.
Multivariable-adjusted models showed incident use of TNF inhibitors correlated with a greater risk for decline in eGFR compared with nonuse (adjusted HR = 1.34; 95% CI, 1.18-1.52). However, anti-TNF use was not associated with risk for all-cause mortality (aHR = 1.02; 95% CI, 0.86-1.21).
Sensitivity analyses yielded similar results, researchers reported.
“Incident use of TNF inhibitors was independently associated with higher risk of progressive kidney function decline but was not associated with risk of all-cause mortality,” Sumida and colleagues wrote. “Further studies are needed to confirm findings and to examine potentially distinct pathophysiologic contributions of incident TNF inhibitor use to kidney and non-kidney outcomes in patients with IBD.”
Sources/Disclosures
Collapse
Disclosures:
Sumida reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures.